Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.5.2.2 Transendothelial Penetration, Bruising and Edema
Transendothelial penetration may involve either the injection of medical nanorobots into the luminal space of a blood or lymphatic vessel via an injection carrier, or alternatively the migration of nanorobots under their own power out of a blood or lymphatic vessel into the tissues or out of the tissues into a blood or lymphatic vessel.
Injections of nanorobots directly into blood vessels (Chapter 16) should produce minor localized disturbances to just a small number of vascular endothelial cells. The metamorphic hypodermic injection carrier can maintain a tight seal throughout the injection process. Rather than relying on natural endothelial lesion repair mechanisms that may take many weeks to complete in the case of a traditional large-gauge hypodermic needle [3758, 3759], the vascular breach due to a nanomedical hypodermic carrier is cellularly resealed immediately post-injection. Fluid leakage, bruising and edema should be negligible.
Incautious or reckless migration by medical nanorobots from a blood vessel lumen through vascular walls into the tissues, called transmigration, extravasation or diapedesis (Section 9.4.4.1), could produce unwanted pathologies ranging from minor bruising or ecchymosis (usually not causing serious pain [4740, 4741]), to localized hematomas, to (in the most extreme case imaginable) massive hemorrhages comparable in severity to the hemorrhagic fevers [3760] caused by filoviruses such as Ebola and Marburg [3761] or (analogously) to cases of full thickness dermal necrosis following extravasation of chemotherapy [5693] or other [5694] agents. These outcomes should be avoidable with good design, including membrane sealing protocols during intercellular passage (Section 9.4.4.3) and attention to avoidance of unintentional mechanical cytocide (Section 10.4.2).
Reverse diapedesis [3762, 3763] or intravasation [3764], from tissues to vascular compartment, also may be undertaken by medical nanorobots analogously to living cells [3762-3765]. Under normal circumstances, nanorobot diapedesis including endothelial gap widening, nanorobot extravasation or intravasation, and gap resealing, should be accomplished in some tens of seconds (Section 9.4.4.1). If the gap between parted endothelial cell junctions and the exterior surfaces of the transiting nanorobot is held to 1 micron or less, then platelets, red cells,* and white cells cannot escape from the vascular compartment during diapedesis. This virtually eliminates any possibility of bruising or hemorrhage and greatly limits the potential for thrombogenesis, inflammation or pain at the site of histopenetration. Transdermal injections of nanorobots (Chapter 16) channeled directly into tissue compartments using sensor-tipped metamorphic needles can actively avoid all vascular penetrations, again virtually eliminating any possibility of the local bruising that was common with 20th century hypodermic rigid needles.
* During erythrocyte diapedesis, red cells can sometimes pass through endothelial wall openings as narrow as 0.5 microns [2755].
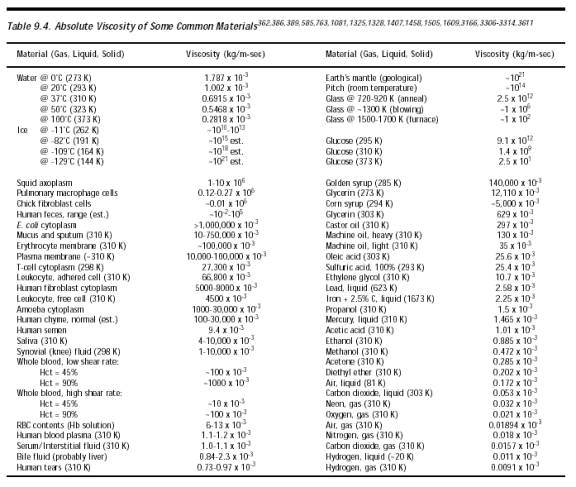
Typically more than 70% of the water of the blood is exchanged with extravascular water every minute (~35 cm3/sec whole-body) – the walls of smaller capillaries are veritable sieves with respect to water (Section 8.2.1.2) – and about 20 liters/day (~0.2 cm3/sec whole-body) of free water leave the circulation via ultrafiltration through leaky capillaries. Of this amount, 18 liters/day are reabsorbed after passing through the lymphatic capillaries and back into the venous loops, leaving ~2 liters/day to pass onward through the lymphatic system (Section 8.2.1.3). If the mean endothelial-nanorobot gap during the entire transit event is equivalent to a pipe of radius 0.1 micron, length 10 microns, and assuming a histoarterial pressure differential of ~0.1 atm (76 mmHg) for plasma fluid of viscosity 0.001 kg/m-sec (Table 9.4), then from Eqn. 9.25 the Poiseuille plasma fluid flow through each diapedetic gap is at most ~40 micron3/sec. In the worst-case scenario, the simultaneous parallel transit of 1012 nanorobots past the ~1012 endothelial cells of the human vascular tree (Section 8.2.1.2) releases an additional ~40 cm3/sec – or roughly the normal extravascular water exchange rate – during the nanorobot fleet transit which may last only some tens of seconds. Total systemic fluid leakage volume during this scenario is 0.5-1 liter (1-2% of total body water, 9-18% blood volume or blood pressure reduction). This is far less than the hourly lymphoplasmatic circulation, and blood hematocrit temporarily rises from 44% to 50-55% in human males, all of which seems tolerable in healthy patients. (A packed cell volume >~55% is the recommended clinical threshold requiring therapeutic bloodletting during apparent polycythemia [3766].) However, the tolerability will depend largely on the fluid status of the patient (e.g., hypovolemic or euvolemic) and on the patient’s cardiovascular status (e.g., how well the heart can compensate for a decrease in blood pressure and volume). In each case, it will be important to assess the patient’s health status and evaluate the medical risks, however small, of a nanorobotic procedure – as nothing is totally without risk.
Nanorobot-induced vascular leakage could be pathognomically similar to: (1) fluid retention syndrome [3767] or idiopathic edema, which can produce symptoms of bloating, fatigue and generalized weakness, headaches, blurring of vision, abdominal pains and diarrhea, and (possibly psychosomatic) signs of fibromyalgia [3767]; (2) contracted plasma volume syndromes (relative polycythemias) [3768]; (3) vascular leak syndrome [3769] during immunotherapy, with more serious effects; or (4) other systemic causes [5894]. However, patients with high-altitude sickness experience changes in total body water* ranging from 4.7% [3770] to 18% [3771] with an elevated hematocrit >62% [3771]. Edematous patients with chronic severe anemia have body water 14% above normal [3772]. Untreated patients with chronic limb edema [3773], severe clinical edematous congestive heart failure [3774], or edematous obstructive pulmonary disease [3775] may have body water 13%, 16% or 21% above normal, respectively. By comparison, a worst-case nanorobot-induced 1-2% change in total body water distribution that persists for perhaps some tens of minutes seems unlikely to prove troublesome. Syncope due to the 9-18% reduced blood pressure (hypotension) also appears unlikely. In one hyperbaric experiment [3776], a transient ~50% circulatory depression in which arterial pressure fell from 120/80 mmHg down to 60/53 mmHg in just 20 seconds did not cause the healthy young adult subject to lose consciousness or significant mental capacity, and C. Wiley notes that ER or OR patients with systolic pressures in the 70s are often conscious. Another experiment [3777] on children exhibiting unexplained syncope found an average blood pressure decline of -45/23 mmHg (-40%/30%) after moving from supine to upright posture, with a 27.7 sec recovery time compared to 16.5 sec for normal children. Yet another study [3778] of postprandial hypotension in elderly subjects found a mean reduction of –30 mmHg (-25%) following an oral glucose tolerance test, with only one of the five subjects reporting a brief episode of light-headedness. Again, it is worth noting that many of the patients receiving nanorobotic procedures may not be healthy young adults, so extrapolation of the data to other populations should be done with caution; it is essential to identify the health status of the patient prior to performing a nanorobotic procedure.
* These shifts, though compensatory for decreased atmospheric pressure and decreased oxygen availability and not due to vascular leakage, may suggest potentially useful thresholds for leakage tolerance.
Fortunately, most therapeutic applications may allow local vascular transit rates 1-2 orders of magnitude lower than the worst-case scenario described above, or may involve significantly smaller nanorobot populations in transit. The overall conclusion is that fluid leakage through temporary vascular breaches induced by extravasating or intravasating medical nanorobots can be made acceptable and largely nonedematous, nonhemorrhagenic, and insensible to the patient. It is important to note the risk of passage of some bacteria and viruses between blood and tissue compartments during nanorobot histopenetration. Such risks, although realistically unavoidable whenever tissue barriers are breached, appear to be much reduced when such methods are compared with conventional hypodermic needles.
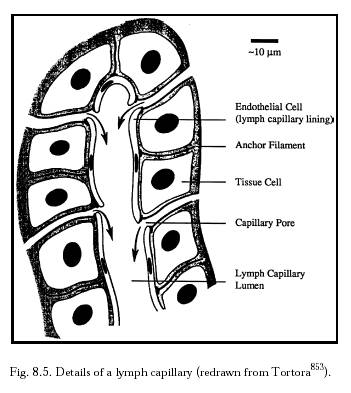
Elevated interstitial colloid osmotic pressure – most severely, due to blockage of the lymphatics which prevents the normal return of proteins to the circulation – can also cause high interstitial fluid pressure and edema [5893]. Proteins that would normally leak through capillary walls gradually accumulate in the tissue spaces until the interstitial colloid osmotic pressure approaches the plasma colloid osmotic pressure, whereupon the capillaries lose their normal osmotic advantage of holding fluid in the circulation so that fluid now accumulates abundantly in the tissues [5893]. Guyton [5893] notes: “Lymphatic blockage commonly occurs in the South Sea Island disease called filariasis, in which filariae (a type of nematode worm) become entrapped in the lymph nodes and cause so much growth of fibrous tissue that lymph flow through the nodes becomes totally or almost totally blocked. As a result, certain areas of the body, such as a leg or an arm, swell so greatly that the swelling is called ‘elephantiasis.’ A single leg with this condition can weigh as much as the entire remainder of the body, all because of the extra fluid in the tissue spaces.” Care must be taken to avoid analogous lymphatic blockages by large numbers of medical nanorobots passing through, temporarily parked in, or geometrically trapped in prelymphatic pores (Figure 8.5, Section 8.2.1.3) in large tissue regions, or in the lymph nodes – that is, nanorobot-induced lymphedema [5895-5899]. Inflammation (Section 15.2.4) or granulomas (Section 15.4.3.5) of the lymphatic channels due to the presence or passage of medical nanorobots, if not avoided by good device and mission design, could also result in nanorobot-induced lymphangitis with edema [5900-5902] and fibrosis [5903], with exacerbation of certain infections [5904].
Last updated on 30 April 2004
{kind=link}
{kind=link}