Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.1.2 Mechanical Damage from Inhaled Diamond
As with ingested diamond dust, inhaled microscopic nanorobots (Section 15.4.3.3.3) or other diamondoid particulates might do serious mechanical damage to lung tissues. (MEMS researchers such as Kaigham Gabriel at AT&T Bell Laboratories have already reported the accidental inhalation – evidently harmless – of silicon micromachines [110].) It has long been known that abrasive dusts can increase the incidence of upper respiratory tract diseases, and fibrosis-inducing dusts can lead to chronic lung ailments [167]. Fiber health science commonly focuses on particle dose, dimension, and durability [6061]. World Health Organization (WHO) antipollution guidelines specify a maximum allowable exposure of 0.23 mg/m3 of total suspended particulate matter (SPM) for no more than 7 days per year [168], consistent with human health. The Swiss national standard is an annual mean SPM of 0.07 mg/m3, though an increase in respiratory symptoms and some decrease in lung function has been observed [770] for chronic exposures as low as 0.014-0.053 mg/m3. In the 1990s, most Western cities were measured at ~0.05 mg/m3, while most major third world cities were measured at ~0.20 mg/m3 [169, 515]. In 1996, the U.S. EPA proposed new particulate matter standards for <2.5-micron particles (PM2.5) of 0.015 mg/m3 for the annual mean and 0.050 mg/m3 over a 24-hour period [170]. (A Health Effects Institute study in 2000 found 0.5% increase in death rates per 0.010 mg/m3 increase in PM2.5 [2172].)
An SPM of 0.10 mg/m3 consisting entirely of 1-micron3 diamondoid flying nanorobots (Section 9.5.3) of mass density ~1000 kg/m3 would represent a number density of ~10 million particles/m3. By comparison, quiet country air (absent any local mining activities) has ~20 million particles/m3 [167], residential city air perhaps 60 million/m3 [167], the worst congested downtown city air ~150 million/m3 [167], and a room with smokers present ~270 million/m3 [896] or more. In 1999, laminar flow clean rooms in a Class One semiconductor fab plant had air with only ~10 particles/m3 of size 0.5 microns or larger [896]. Experimental data suggests that a condition of lung overload occurs when the retained lung particle burden reaches a particle volume of ~109 micron3 per gram of lung tissue (e.g., ~0.1% by volume) [781].
A resident of an industrialized Western country typically inhales ~30 billion particles per day [6061]. A cubic meter of ordinary air likely contains ~10,000 grains of pollen and fungal spores, as well as carbon monoxide, radon gas, scent molecules, spider legs, fragments of soil, fur, a bit of carbon from a faraway fire, dust mites from the carpet, flakes of skin, hair and lint particles, bacteria and viruses, up to 1011/m3 nanometer-sized particles in urban air [6197], sea spray wave-produced ultrafine salt particles near the coasts [6179], and even wisps of 15-micron-wide droplets from when someone last sneezed [896] – often with a thin coating of hydrocarbon molecules (esp. fossil fuel combustion products). It is universally recognized that continued inhalation of certain dusts is detrimental to health and may lead to reticulation of the lungs and eventually to fatal diseases included under the general term pneumoconiosis [171, 172]. Coal and silica dusts are particularly harmful. Chronic inhalation of crystalline silicon dioxide particles measuring 0.5-5 microns in size can lead to silicosis [173, 174], a chronic inflammatory lung disease that can ultimately destroy the ability to breathe.
Fine particles in the micron size range, typical for dust inhalation hazard, can bypass the mucociliary (e.g., cilia in the respiratory epithelium; Sections 8.2.2 and 15.4.3.3.3) and cellular defense mechanisms, invading the lung parenchyma and causing an inflammatory response. Nasal turbulence ensures that almost no particles larger than 2-5 microns reach the lower airway [2495] (Section 8.2.2); these larger particles are deposited by inertial compaction at airway bifurcations, hence are easily flushed out via bronchial mucus flow. (The airstream turns abruptly, and particle inertia carries it straight on against the airway wall [173].) However, these large particles can be inhaled orally, with experimentally-determined [5023] retention rates of 46-56% after 24 hours, and 25-31% after 21 days, for 6-micron Teflon particles inhaled rapidly or very slowly, respectively.*
* In hamster lungs, inhaled 5.5-micron Teflon microspheres show maximum retention after 21 minutes in alveoli (72.4%), less in intrapulmonary conducting airways (22.9%), and the least in extrapulmonary mainstem bronchi (0.3%) and trachea (4.4%) [5027]. The Teflon particles were found submerged in the aqueous lining layer and in close vicinity to epithelial cells. In intrapulmonary conducting airways, 21.5% of the microspheres had been phagocytized by macrophages, a fate made possible by the displacement of particles into the aqueous phase by surfactant [5027].
Particles smaller than 0.5 microns generally remain airborne and are exhaled, though a few may be deposited in the alveoli* [173]. There also is much evidence that some particles which are nontoxic in micron sizes may be toxic in the nanometer range [761, 769, 929-933, 4846, 4858]. For instance, the intensity of neutrophil alveolitis is lowest for 260 nm carbon particles, higher for 50 nm particles, and highest for 14 nm particles at low doses up to 0.5 mg/kg where particle reaction is governed by surface area effects [769]. However, at larger doses sufficient to induce lung overload, the larger particles become more inflammogenic per unit mass or volume [769].
* Certain very small submicron particles may be trapped in the alveoli. For example, technegas [661-668] is an argon gas-suspended Tc99m labeled 5-200 nanometer [661] carbon-particle radioaerosol developed for diagnostic lung imaging that is well tolerated by patients [662, 663], with over 100,000 clinical studies by 1993 [664]. It was once suggested that technegas particles might be C60 molecules each containing a single endohedrally-trapped technetium atom [665], but TEM, SEM, and AFM imaging found that this radiopharmaceutical consisted of hexagonal mostly 30-60 nm platelets of metallic Tc99m encapsulated within a thin layer of graphitic carbon [666]. Traditional dry insoluble technegas particles adhere well to alveolar walls upon inhalation (after a single-breath diagnostic dose [667]), whereas pertechnegas particles, which have no carbon coating, rapidly disappear from the lungs via exhalation [668].
In the mining, quarrying, ceramic and abrasive industries, the acute danger limit (e.g., the minimum toxic dose) is reached when ~200 million particles/m3 of free silica are present in air, with sizes below 5 microns. Of these, as many as 25% are retained in the respiratory tract [167]. Unfiltered 20th century airborne industrial dusts typically would consist of ~20% of particles below 1 micron, ~70% between 1-3 microns, and ~10% over 3 microns in diameter [167].
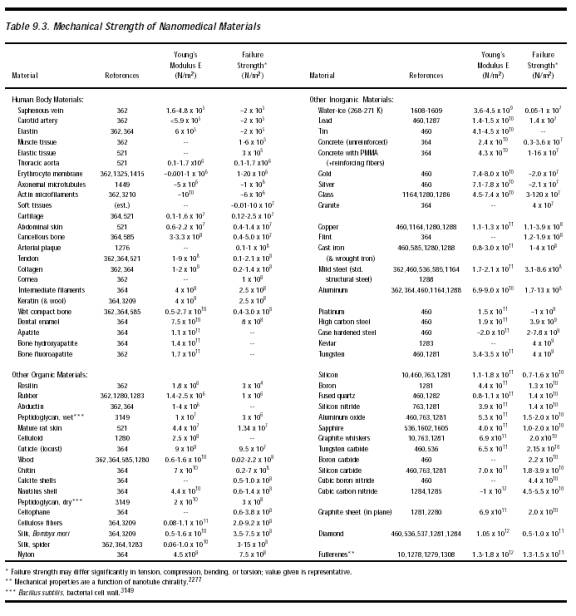
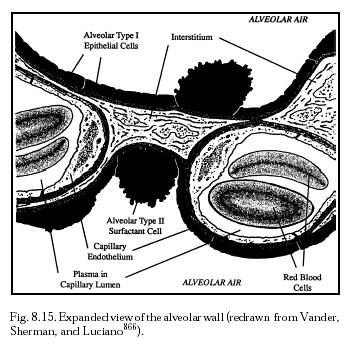
Like diamond, pure silica has a tetrahedral crystalline lattice that cleaves similarly, potentially making hard shards (Table 9.3) of comparable sharpness, and thus possibly displaying similar mechanical effects on human lung parenchyma. Particles 0.5-5 microns in size that reach the lower respiratory tract are deposited in small airways and along the surfaces of alveoli deep inside the lungs [173]. Many silica crystals penetrate the respiratory epithelium, lodging in the interstitium between cells (Figure 8.15), and eventually worm their way into the lymphatic channels and progress into the lymph nodes [173]. About 20% of these insoluble crystals are never cleared from the body (Section 15.4.3.3.3). At the site of each intrusion, a lesion develops, probably due in part to the chronic mechanical irritation, leading to tissue inflammation, the formation of “silicotic nodules,” fibrosis and scarring [175]. (Inhaled insoluble tungsten particles have also been found in mediastinal lymph nodes (Section 8.2.1.3) of workers with hard metal lung disease [176].)
Alveolar macrophages engulf and ingest silica crystals that reach the alveoli. Once inside the cell, the crystal sets in motion a sequence of biochemical reactions (especially involving reactive oxygen molecular species) that ultimately destroys the cell, causing it to rupture and release its intracellular enzymes and the silica crystal back into the surrounding lung tissue. (See also footnote, Section 15.6.3.4.) The enzymes damage the lung tissue, which subsequently heals by fibrosis. This silica particle is re-phagocytized by another macrophage, and the cycle repeats; the end result of this process is respiratory failure [177]. (Neutrophils are also present, typically ~6 x 104 cells per gram of wet tissue in mammalian lungs [763].) One study suggested that as little as 1 milligram of 5-micron silica crystals inhaled per 100 grams of body weight is enough to kill a rat by producing a severe alveolitis and fatal pulmonary edema. Indeed, within 24 hours of the lethal exposure researchers observed “gasping, cyanosis, and discharge of a pinkish and frothy fluid from the mouth and the nostrils” among the rodents prior to death [175]. The equivalent exposure at a 70-kg human body weight, all else equal, would require the inhalation of ~0.7 gm of 5-micron silica dust – roughly the same volume as ~3 billion inhaled 5-micron airborne silica crystals.
Pneumoconiosis from exposure to artificial graphite made from coke has not been reported and probably occurs only rarely [670]. A survey of over 600 cases of graphite pneumoconiosis [673] yielded just one case in which nearly pure graphite might cause graphite pneumoconiosis. The majority of the evidence indicates that pneumoconiosis is a mixed-dust lung reaction, and that analytically pure graphite probably does not cause pneumoconiosis [673, 674, 675]. Silicographitosis has been documented following excessive exposure to natural graphite (plumbago) in graphite mines [671], which is a crystalline form of carbon containing free silica [174]. Carborundum fibers, a synthetic abrasive made by fusing silica and carbon, also produce fibrosing alveolitis [672]. The most common carbonaceous-hazard diseases include anthracosis and emphysema (coal) [178], graphitosis (natural graphite), and smog lung (carbon plus photochemicals). Federal regulatory limits on coal mine dust (predominantly elemental carbon with a maximum of 5% silica [179]) are 2 mg/m3. Subchronic inhalation of 1.1 mg/m3 of carbon black dust is not mutagenic or genotoxic for rat alveolar epithelial cells and elicits no detectable adverse lung effects [761].* Subchronic inhalation of carbon fibers at 20 mg/m3 also has no injurious effect on rats [765]. Bronchiolar (large-particle) coal dust is quickly cleared via the mucociliary escalator (Section 8.2.2). Smaller alveolar-resident particles are mostly taken up by macrophages, which migrate over the airspace surface to the terminal bronchioles, then enter the mucociliary stream [179]. Within ~2 hours post-exposure, ~2% of these particles penetrate the airway lining and enter the interstitium (Figure 8.15) and the phagocytic vacuoles of lymphatic endothelial cells; at 24 hours, the particles are detected in the peribronchial lymphatics and lymph nodes [180]. Pure carbon particles can also insinuate themselves permanently into the skin [181].
* The American College of Governmental Industrial Hygienists has set a threshold limit value of 10 mg/m3 for nuisance dusts and 3.5 mg/m3 for pure carbon black dust, but this is based on avoidance of excessive workplace dirtiness and not on the toxicity of carbon black per se [764].
More than 3000 naturally occurring minerals are known to present a respiratory hazard [167], including aluminum [182, 958], asbestos [183], barium [184], beryllium [185, 186], germanium [187], iron [188], molybdenum [189], talc [190-192], and tin [193]. Even the aspiration of common table pepper particles has proven fatal in children [194, 195]. Exposure to 9- to 24-micron diameter glass fibers (e.g., synthetic vitreous fibers or SVFs) such as are found in fiberglass insulation [196] can produce a transient irritation of the mucous membranes of the eyes, nose, and throat [197] though no long-term adverse effects such as lung fibrosis, lung cancer, or mesothelioma has been shown [198, 199]. However, very long [758, 759] and thin glass fibers (diameter < 1.5 micron) are cytotoxic in vitro [757] and highly carcinogenic after intrapleural implantation [200] inducing malignant mesothelioma and fibrosis in rats [2493]. Fiberglass dermatitis is well known [201]. Adverse pulmonary effects are a function of dose, dimensions, and durability of fibrous particles [2494]. Interestingly, even “healthy” human lungs are loaded with inorganic microfibers – a lung tissue biopsy of 10 normal subjects found 1.5 x 106 fibers/gm, as compared to 141.9 x 106 fibers/gm in the lungs of 11 asbestos-exposed individuals, with fiber length most commonly 3-5 microns in both groups [202].
But what about diamonds? A recent (2002) review of the modern medical literature revealed no explicit reports of diamond dust inhalation toxicity, nor was this possibility even mentioned in any of the standard reference works. Potential risks from the airborne release of inhalable diamond dust into the oral cavity from dental drills during common clinical use appears not to have been widely investigated, despite data showing that particles can be thrown up to 90 cm from the patient’s mouth and may remain suspended in the air for hours [203]. (Minor risks to dental personnel due to simultaneous metals exposure [115] or silica [204] have been considered.)
However, there is at least one suspicious case study [205] involving five Belgian diamond polishers that could possibly represent an instance of undiagnosed respiratory diamond poisoning. In the Belgian gem-finishing occupations, workers use high-speed diamond-cobalt grinding tools to polish diamonds that have already been cut. The grinding surface is a spinning wheel consisting of 20- to 40-micron diamonds cemented onto a layer of fine 400-mesh ~64-micron cobalt metal grit. During grinding and polishing, cobalt grit and microdiamonds are abraded from the wheel and are thrown into the air, then inhaled by the workers.
In 1984, eight physicians at the Clinic of Medicine of the Catholic University in Leuven, Belgium, treated five individuals (non-smokers) for interstitial lung disease or fibrosing alveolitis. This condition is normally reversible with proper treatment. Symptoms included painful breathing, crackling noises coming from the lungs, coughing and wheezing, chest tightness, runny nose, and weight loss. But the condition was puzzling because no case of lung fibrosis had ever been attributed to cobalt powder exposure alone.
Could the disease have been caused by respiration of airborne abraded microdiamonds? The physicians did not investigate this possibility and concentrated instead on the more familiar cobalt culprit – “intoxications by cobalt alone [would] be enlisted as a compensatable industrial lung disease.” Lung tissue biopsies showed no “massive tissue necrosis,” and the journal report is silent as to whether or not there was any search for evidence of microdiamonds in lung tissue – despite the clue, perhaps more clear in retrospect, that fume hoods over the work stations were reported to contain large amounts of “amorphous carbon” besides the cobalt particles. The physicians finally ascribed the disease to cobalt, even though, according to the case histories, 3 of their 5 patients were clearly not healed, years later, despite having received the correct treatment for cobalt poisoning. Could this be a case of undiagnosed diamond dust injury?
First, over the last two decades numerous studies have conclusively proven that pure cobalt is at worst a mild irritant and does not appear to cause lung fibrosis by itself [175, 206-209, 212, 213]. Gennart and Lauwerys [210] question the role of cobalt alone in producing lung fibrosis and note that “the possible interference of other components of the dust inhaled by the workers who developed the disease remains to be elucidated....There is suggestive evidence that other components of the inhaled particles interfere with the biological reactivity of cobalt on the lung.” Lauwerys and Lison [211] note that industrial exposures to cobalt commonly include “other substances such as tungsten carbide, iron, and diamond, which may modulate the biological reactivity of cobalt [emphasis added].” Others [212], including the lead author of the Belgian study [213], now implicitly acknowledge that microdiamonds could be medically relevant.
Second, other studies have suggested that the presence of carbides, particularly tungsten carbide, can interact with cobalt to produce the observed fibrosis [175, 208, 214, 215], but in the case under discussion the investigators specifically reported that “no measurable amounts of carbides of tungsten or other metals were present....Cobalt was, besides the microdiamonds, the almost exclusive component of the grinding surface of the disks.” [205] Limited studies in hamsters show that intratracheally-instilled cobalt (5 mg/kg) and diamond particles (50 mg/kg) caused more acute lung damage then when these particles are administered alone [213]. So the original conclusion of the Belgian diamond-polishers alveolitis study – i.e., that cobalt alone caused the problems – might well be invalid. The specific possibility that diamond dust could have been involved remains unaddressed.
A related study of three additional diamond-polisher patients (including two smokers) who presented with bronchial asthma alone [216] probably was correctly attributed to the cobalt [209], and there are other similar cases [4739]. But another case involving a single diamond-polisher patient (a smoker) who presented with both bronchial asthma and alveolitis [217], also attributed to the cobalt, is of uncertain validity – as yet, no studies have focused on diamond as a possible contributory factor. An autopsy of lungs of hard-metal grinders revealed the frequent presence of corundum but no specific search for diamond particles was reported [218]. Vital capacity was found to be significantly impaired among young workers who were exposed to “carbon dust” during diamond cutting and polishing in India [219], and in 2002 increased lipid peroxidation was reported in miners working in the diamond extraction industry in Yakutia, Russia [4737]. A 62-year-old Japanese patient who had been a diamond-grinder for 20 years showed numerous unusual well-circumscribed tumors on the parietal pleura, diagnosed as pleural plaques [220], and 0.1- to 0.6-micron spherical carbon-black particles (in the virtual absence of quartz) are known to have caused fatal carbon pneumoconiosis in at least one other case [181].
On the positive side, Schmidt et al [221] specifically assert that diamond dust is nonfibrogenic in human monocyte-macrophages (“dust cells”) found in the lungs. Hedenborg and Klockars [222] used diamond dust as an “inert control” in their experimental work, and found that diamond dust did not stimulate the production of reactive oxygen metabolites by polymorphonuclear leukocytes – a proposed pathway for chronic inflammation and tissue injury of the lung. Inhalation experiments with rats and guinea pigs indicate that dust from carbon fibers produces no systemic toxicity or pathological changes in the lungs [223, 224, 765], and medical examination of carbon fiber production workers has revealed no adverse effects on the lungs [225], though one Russian animal study found slight pulmonary fibrosis and respiratory tract irritation from carbon fiber dust [226] and a Japanese study found morphological changes in rat lungs due to some kinds of carbon fibers [762]. But none of these results allow us to rule out the possibility of mechanical damage to lung tissues by ragged diamond shards (Section 15.1.1).
Although there is no direct evidence of any harm, a conservative appraisal would appear to warrant a careful study of the lung toxicity of fractured diamondoid detritus. Because of the likely importance of sapphire in nanodevice design, crystalline corundum and emery [227-229] (e.g., grinding grits) probably should also be investigated for both ingestion and inhalation mechanical toxicity. (See also Section 15.3.5.5.)
Last updated on 30 April 2004
{kind=link}
{kind=link}