Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.3.5.5 Alumina and Sapphire Particles
The biocompatibility of alumina and sapphire particles has been investigated because it is important to understand the biological reaction to inhaled particles and to wear particles that might be produced by frictional forces in long-term prosthetic implants. Such studies generally involve micron-scale particles, roughly the size range of future medical nanorobots.
First, is alumina powder lethal? Massive administration of several bioactive <44-micron ceramic powders were lethal to Balb/c mice in 5 gm/kg doses when injected intraperitoneally, producing a swollen kidney having an ischemic color, with edema of interstitial tissue in the kidney cortex, severe degenerative changes in the tubular epithelial cells, and hyaline deposits in the renal collecting tubules, along with edema and inflammation in pulmonary tissues [1067]. Nonbioactive alumina powder similarly injected as a control (equivalent to 90 trillion 1-micron3 nanorobots injected into the peritoneal cavity of a 70-kg human) was not lethal and elicited no significant changes in blood chemistry, though there was some loss of body weight [1067]. All powders had almost no systemic effects when injected intramuscularly or subcutaneously [1067]. IP-injected particle pathogenesis was believed to derive from phagocytosis by lymphocytes and macrophages, leading to release of lymphokines and free radicals that could damage kidney, lungs, and liver, with small amounts of bioactive ceramic powder being removed rapidly from the peritoneal cavity. Ceramics in fine powder form are generally believed to have higher bioactivity and to be associated with higher mortality. In this experiment [1067], as ceramic particle size was increased the fatal effects in mice decreased. Consistent with their extremely low water solubility in the near-neutral pH range (Section 15.3.5.6), aluminas are minimally absorbed from the essentially aqueous intestinal contents, and for the same reason are blocked from absorption through the skin [958].
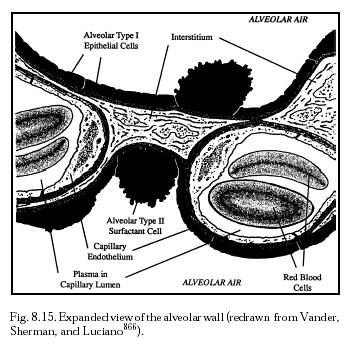
Early studies [1050] of 0.5- to 5-micron alumina particles implanted subcutaneously and intraarticularly (knee joint) for up to 5 months in mice revealed no persistent inflammatory or progressive fibrotic reactions around the powder deposits. After an initial acute (3-7 day) granulocytic inflammatory phase, the material was gradually contained within macrophages and deposited locally without significant fibrous tissue reaction. Some particles were transported via lymphatic vessels into regional lymph nodes [1050]. Particles were found in the interstitium of the lung (Figure 8.15); in the reticuloendothelial cells of the liver, spleen, and bone marrow; and in one case in the meshwork of a renal glomerulum; but rarely in the bloodstream. Such crystal deposits caused no local cell necrosis, fibrosis, or granulomatous reaction in any of these organs [1050].
Rat tissue responses to alumina powder administered at low doses were investigated by Di Silvestre et al [1068], who found that powdered alumina implantation in the subcutis, the muscle and the peritoneum of the rat produced the same intense acute inflammatory reaction in all implantation sites after 2 weeks. However, after 8 weeks the inflammatory reaction had regressed and there was a thin layer of connective tissue around the implanted material, completely isolating it from the surrounding tissues [1068]. Examination of human biopsies from well-fixed human total hip prostheses showed that alumina particle deposits increase with time with only a low-grade macrophagic reaction. An inflammatory reaction appeared when joint loosening occurred, but this reaction was less striking than with loose metal-polyethylene prostheses [1069]. The amount of necrosis and fibrosis was lower for alumina implant wear debris than that associated with metal or polyethylene implants [973]. Intraperitoneal and intramuscular implantation of powdered alumina particles in rats showed an initial granulocytic reaction with some uptake by the reticuloendothelial system [1053]. Intra-articular injection of alumina wear particles into rat knees revealed a correlation between the numbers of particles and the macrophage response in the tissues. At 1 week the macrophage response to Co-Cr particles similarly injected was significantly greater than for the Al2O3 particles, possibly due to the necrosis of macrophages induced by Co-Cr particles [1070]. No antigenicity of alumina ceramic was found in another study that attempted induction of footpad swelling in ceramic-immunized mice [1048]. Histopathological studies of alumina powder applied to dog tooth wounds have been reported [1071].
Most cytocompatibility studies of alumina particles have examined the foreign-body reactions of macrophages [1106]. For example, it is known that rat alveolar macrophages readily ingest aluminum oxide particles [862, 1053]. Toxicity tests of alumina powder in vitro using rabbit alveolar macrophages and in vivo using direct intratracheal injection into rat lungs found that the powder had low toxicity for macrophages and minimal recruitment of airway cells and neutrophils in the rat lungs [845], although soluble aluminum salts employed as vaccine adjuvants may have been implicated in macrophagic myofasciitis [1752].
Sapphire is generally biocompatible with macrophages. Pizzoferato et al [1077] found that saline-suspended 1- to 12.5-micron alumina particles were only slightly phagocytosed in vivo by mouse peritoneal macrophage cells lavaged 1 week post-injection. Harms and Mausle [1053] tested the biocompatibility of alumina ceramic in macrophage cultures and found no acute cytotoxicity. Christel [973] noted that an examination of human biopsies from failed total hip prostheses revealed a foreign-body reaction containing predominantly macrophages, loaded with alumina particles, that had no morphologic alteration and had not lost their chemotactic ability [973] – though one more recent study found that macrophages grown from monocytes in the presence of alumina were somewhat negatively affected [1072]. In another study by Rader et al [1073], human monocytic THP1 cells were differentiated over a period of five days in the presence of vitamin D3 and GM-CSF in macrophage-like cells in the presence of various particles and concentrations. The secretion of tumor necrosis factor (TNF) – considered to be the initiator protein of particle disease leading to aseptic loosening of endoprostheses – was measured and was found to be elevated 4 times control for alumina ceramic particles, compared to 23 times the control level for polyethylene particles and 25 times control for cobalt particles. Nakashima et al [1103] reported that 1-, 100-, and 1000-micron alumina particles could induce the release of bone resorbing mediators (IL-6, TNF-alpha, IL1-alpha) by macrophages in a dose-dependent manner, but hydroxyapatite particles of equal size stimulated a greater release than the alumina. Nkamgueu et al [2596] found that alumina microparticles ingested by human blood monocytes that had been forced to differentiate into macrophages over a 7-day period decreased the macrophages’ intracellular K/Na ratio (a measure of cell vitality), decreased their phagocytic ability by 27%, and reduced their oxidative metabolism by a factor of 5.
Catelas et al [1074] measured the effects of size (0.6- to 4.5-micron), concentration (5-1250 particles/macrophage), and composition (e.g., alumina) of ceramic particles on phagocytosis and cell mortality in the J774 mouse macrophage cell line. Kinetic studies (from 5 min to 24 hours) revealed that phagocytosis of the particles begins very early after cell exposure, increasing with time and particle concentration and reaching a plateau after ~15 hours. Phagocytosis increases with concentration for particles up to 2 microns. For larger particles up to 4.5 microns, phagocytosis reaches a plateau independent of particle size and concentration, suggesting a saturation effect most likely dependent on the total volume ingested [1074]. There was no significant difference in phagocytosis between Al2O3 and ZrO2 at 0.6 microns, though alumina seemed to be more easily phagocytosed than high density polyethylene (HDP) at the same size (4.5 microns) and concentrations. Cytotoxicity studies revealed that macrophage mortality increases with particle size and concentration for sizes greater than 2 microns (to >30% cell mortality). Smaller particles (0.6 microns) cause cell mortality only at higher concentrations, and the mortality is still very low (~10%) [1074]. There is no significant difference in cell mortality and inflammatory mediator TNF-alpha release between Al2O3 and ZrO2. TNF-alpha release increases with particle concentrations and is significantly higher with HDP than with alumina [1074]. Related studies by Catelas et al [1075, 4789] using the same cell model investigated the induction of apoptotic cell death (Section 10.4.1.1) in macrophages by alumina ceramic and other powders of different sizes and concentrations. Of some concern, Catelas found that the apoptotic effect of ceramic particles on nuclear morphology was size- and concentration-dependent, but that alumina ceramic particles induce apoptosis more effectively than polyethylene particles at concentrations of 125-250 particles/macrophage for ~2 hours [4789]. A more recent study by Nkamgueu et al [2400] found slightly decreased cell vitality and a 27% decrease in phagocytic ability in human macrophages that phagocytosed alumina particles.
The responses of a few other cell types to alumina ceramic powders have also been investigated. For example, cultured human fibroblasts exposed to 1-500 µg/cm3 alumina powder showed no cytotoxic effects with cell viability at different exposure times measured by colony formation efficiency, neutral red uptake and colorimetric tetrazolium reduction [1076]. No cytotoxic or antiproliferative effects were induced in fibroblast-like mesenchymal cell monolayer populations cultured in vitro on powdery alumina ceramic [972]. Alumina powders generally induce no cytotoxicity in cell cultures [598] of human gingival fibroblasts or osteoblastlike cells [1107]. Nishio et al [4765] found that the delta-crystal phase of alumina powder promoted greater differentiation in osteoblasts than the alpha-crystal phase when present in a complex composite ceramic. Rodrigo et al [4766] found some change in osteoblast function from 10-micron alpha-alumina particles in human bone cell cultures, and that while both polyethylene and alpha-alumina increase the expression and secretion of IL-6 in human osteoblastic cells, the stimulation is weaker from alpha-alumina at the same particle dose [4792]. Oonishi et al [974] observed no inflammation or cell infiltration for 10- and 100-micron alumina particles implanted in holes drilled in the femoral condyles of rabbits. Dion et al [643] found that the hemolysis eventually initiated in vitro by alumina powder is almost zero.
As for inhalation toxicity, human experience with alumina powders strongly suggests that they are not associated with major specific pulmonary hazards under typical 20th century conditions of occupational inhalation exposure [958, 4816, 4817], though rodent experiments suggest that clearance of alumina particles from the lung is slow [4812]. OSHA occupational exposure limits for alumina dust are 10 mg/m3 (total fraction) and 5 mg/m3 (respirable fraction), respectively, according to the official Material Safety Data Sheets [958]. (10 mg/m3 of sapphire particles equates to ~3 billion/m3 airborne cubic nanorobots, each 1 micron in diameter.) Alumina refinery workers exposed to >100 mg/m3-year of gamma aluminas for >20 years had a 3- to 4-fold excess of individuals with an abnormal forced expiratory volume at 1 second, with abnormal being defined as <80% of the predicted figure, though smoking had a far more deleterious effect on ventilatory capacity [962]. Alpha-alumina 100-700 nm particles have only minimal [963] or no [965] fibrogenic reactivity, and only at doses instilled intratracheally that are massive compared to the amount which could reasonably be inhaled in any one breath. Such massive doses of gamma-alumina in the 20-40 nm size range did produce a fatal fibrosis of the lungs in rats [964]. Corundum dust has no significant effect on the in vitro enzyme activity of alveolar macrophages in the rat [2496]. Intratracheal instillation of 2 mg of alumina silicate refractory fiber in male Wistar rats produces no evidence of pulmonary fibrosis, unlike other fiber materials [4800].
Last updated on 30 April 2004
{kind=link}